
Autonomy
agents plan task sequences, call tools, and act without direct human intervention
a project with Alive Engine
 Alive Engine
Alive Engine IMT-Atlantique · BRAIN
IMT-Atlantique · BRAIN
Around twenty researchers making AI more accessible: less energy, less data, fewer priors on the data. A broad international network, and years of work on large language models and now on agentic AI.
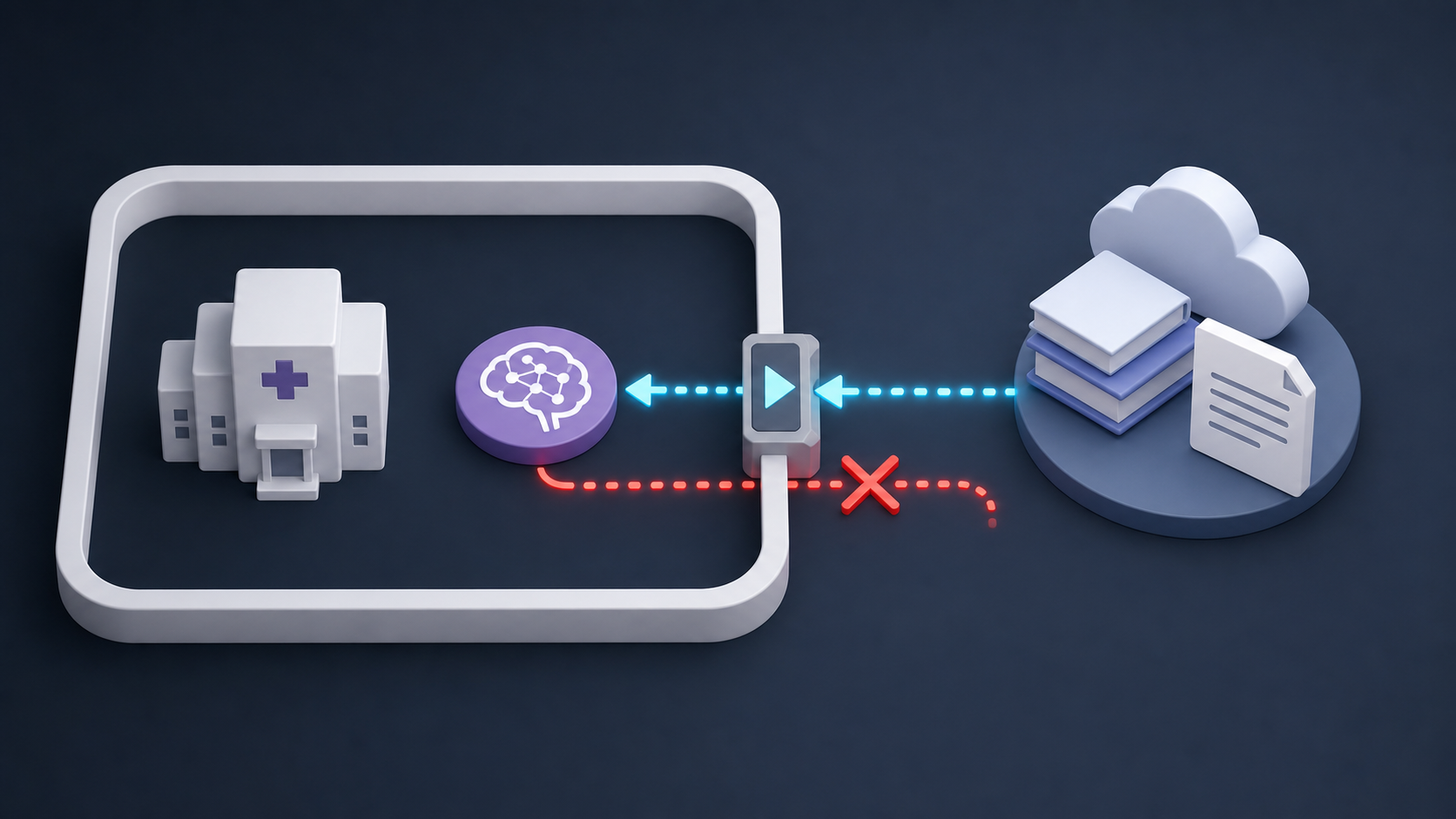
A platform to build, deploy, and supervise persistent AI teammates that learn continuously, accumulate expertise, and work alongside human teams. On-prem for sensitive data, sandboxed, and fully auditable.


phone interface, encrypted thread
agent and server stay inside the hospital perimeter
The project uses Alive Engine as the experimental substrate: continuous tasks, persistent state, introspection cycles, sandboxed execution, and real-time supervision.
agents consolidate what they learn instead of resetting every run
tools, sandboxes, and model calls remain inside the deployment boundary
every action, evidence source, and handoff can be replayed
thresholds, approvals, overrides, and halt states are first-class controls
Questions welcome.
Alive Engine IMT-Atlantique · BRAIN